ACC 2026: CardioAdvocate Take
ACC 2026 Late-Breaking Trials: What Changed, What Didn't, and What It Means for Your Care
A CardioAdvocate Insight Paper
The Bottom Line
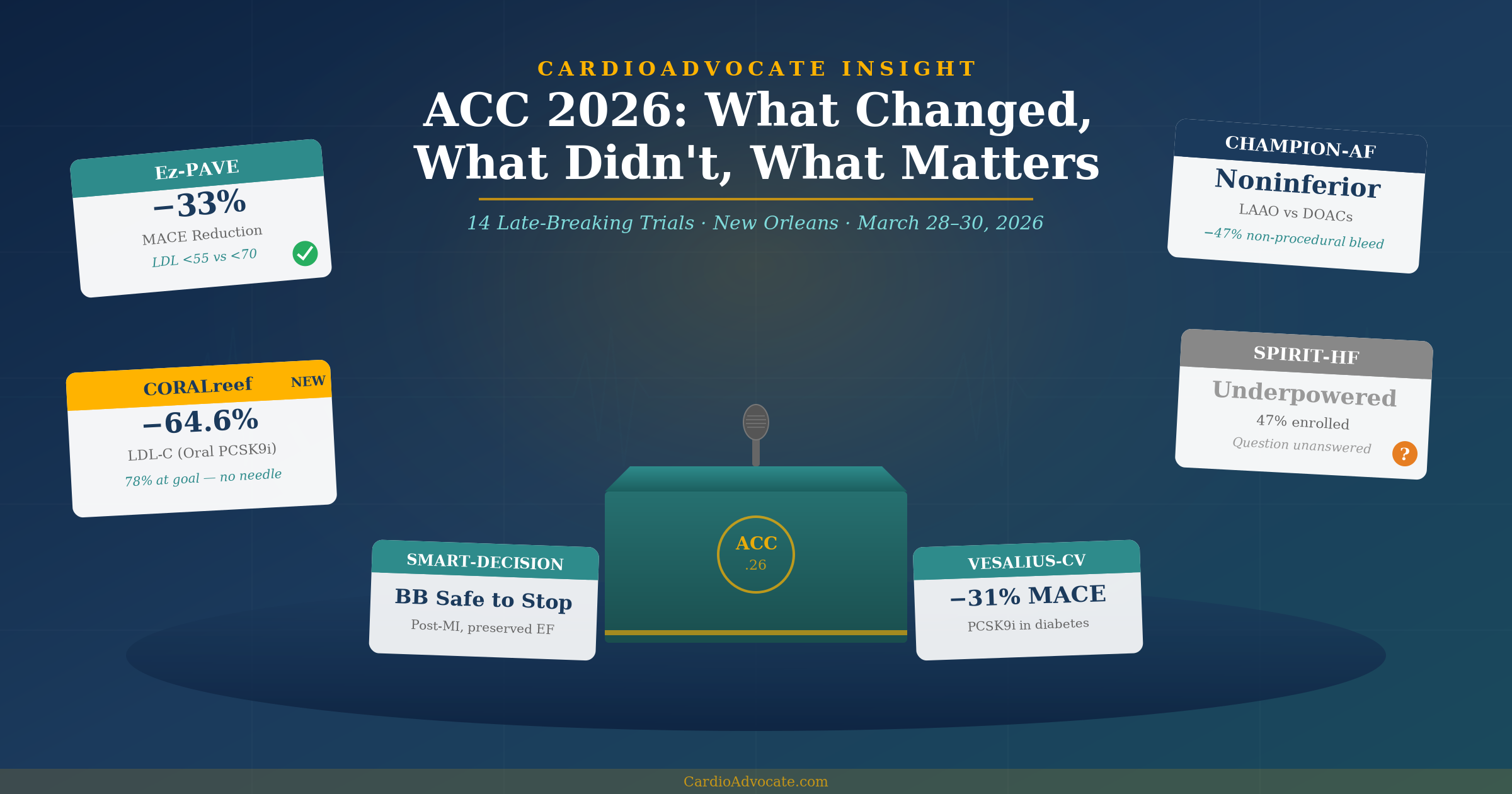
The ACC 2026 Scientific Sessions delivered 14 late-breaking trials across lipid management, atrial fibrillation, heart failure, hypertension, and pulmonary embolism. The collective message is clear: nothing dramatically alters our current position and practice, but rather reinforces it.
These trials provide the randomized controlled trial evidence that many of us have been practicing by for years. Lower LDL cholesterol targets work. Left atrial appendage occlusion has a role — but not as first-line therapy. Beta-blockers deserve scrutiny, not blind adherence. And the question of spironolactone in HFpEF remains, frustratingly, unanswered.
This Insight Paper walks through the major trials, what they mean for clinical practice, and where CardioAdvocate stands on each.
Lipid Management: The Evidence Catches Up
Since its inception, CardioAdvocate has advocated for aggressive LDL-C lowering, earlier intervention, and not settling for "good enough." ACC 2026 delivered the randomized proof.
A trial of 3,048 patients with established ASCVD at 17 South Korean sites, randomized to an LDL-C target of <55 mg/dL versus the traditional <70 mg/dL. At 3 years, the result: a 33% reduction in major adverse cardiovascular events (HR 0.67, 95% CI 0.56–0.82, P < 0.001) in the aggressive arm — driven primarily by fewer nonfatal heart attacks and revascularizations.
This is the first dedicated randomized trial to prove that lower LDL-C targets save lives in secondary prevention. It is no longer a matter of extrapolation from IMPROVE-IT or subgroup analyses. The evidence is definitive.
VESALIUS-CV randomized 12,257 patients with qualifying atherosclerosis or high-risk diabetes — but no prior MI or stroke — to the PCSK9 inhibitor evolocumab (Repatha) versus placebo on top of optimally tolerated statin therapy. Over a median 4.8-year follow-up, the primary endpoint of 3-point MACE was 25% lower with evolocumab (HR 0.75, 95% CI 0.65–0.86, P < 0.001), and 4-point MACE was 19% lower (HR 0.81, 95% CI 0.73–0.89, P < 0.001). This is the first large-scale trial to demonstrate that PCSK9 inhibition prevents first cardiovascular events in a primary prevention population.
A prespecified diabetes subgroup of over 3,600 patients showed an even greater 31% MACE reduction (HR 0.69, 95% CI 0.53–0.91, P = 0.009), with LDL-C driven to 52 mg/dL versus 111 mg/dL with placebo — reinforcing that high-risk diabetic patients derive outsized benefit from aggressive LDL-C lowering. (Diabetes subgroup analysis published simultaneously in JAMA.)
Olezarsen, an antisense oligonucleotide targeting APOC3, achieved 58–64% triglyceride reduction and 72% reduction in remnant cholesterol at 6 months in 468 patients. However, the CTA substudy presented at ACC.26 found no significant change in noncalcified plaque volume at 12 months (P = 0.36) despite the dramatic lipid improvements. Critically, apolipoprotein B was reduced only ~16% — a modest effect that likely explains the disconnect. Plaque is driven by ApoB-containing particles, not triglycerides per se. A 16% ApoB reduction over 12 months is unlikely to produce measurable plaque regression — reinforcing a fundamental principle: any intervention that does not meaningfully lower ApoB-containing particles will not alter the progression of atherosclerosis. Cardiovascular outcomes data from the larger ESSENCE trial program are still needed, but this CTA substudy tempers expectations.
Merck's enlicitide decanoate is the first oral PCSK9 inhibitor to reach Phase 3 results. In CORALreef AddOn, patients on background statin therapy who were not at LDL-C goal received enlicitide as a once-daily oral add-on. At 8 weeks, LDL-C fell 64.6% from baseline — outperforming every guideline-recommended oral non-statin therapy head-to-head: 56.7 percentage points greater reduction than bempedoic acid, 36.0 greater than ezetimibe, and 28.1 greater than the two combined.
Lp(a) decreased 26.2% (compared to an 8.1% increase with bempedoic acid), and 78.2% of patients achieved both ≥50% LDL-C reduction and a level below 55 mg/dL — versus just 2–20% with comparators. Published simultaneously in JACC. The foundational CORALreef Lipids trial (NEJM, February 2026) had already demonstrated a 57% LDL-C reduction at 24 weeks in 2,909 patients versus placebo.
Ez-PAVE is the trial we've been waiting for. CardioAdvocate has consistently maintained that driving LDL-C below 55 mg/dL is the right approach based on the totality of evidence — Mendelian randomization, IMPROVE-IT subgroups, meta-analyses. Now we have a dedicated RCT confirming a 33% MACE reduction. If you or your doctor have been settling for an LDL-C of 68 and calling it "close enough," this trial says otherwise. Lower is better. Start earlier. Don't settle.
VESALIUS-CV extends the picture to primary prevention — and with 12,257 patients and a 25% MACE reduction, the case for early, aggressive LDL-C lowering is now supported by hard endpoints across the entire spectrum from secondary to primary prevention. The diabetes subgroup's even larger 31% reduction underscores the outsized benefit in high-risk metabolic patients. And ESSENCE-TIMI 73b is a reminder that triglyceride lowering alone is not the same as ApoB lowering — if you don't move the ApoB needle meaningfully, the plaque won't budge.
Then there is CORALreef. An oral PCSK9 inhibitor that achieves injectable-level LDL-C reductions — without a needle — changes the conversation about access, adherence, and patient choice. This is not yet FDA-approved, and cardiovascular outcomes data are still needed, but the clinical trajectory is unmistakable. The lipid field is moving forward rapidly, and the barriers to aggressive LDL-C lowering are falling one by one.
Atrial Fibrillation: LAAO Finds Its Place
The largest LAAO trial to date enrolled 3,000 patients with atrial fibrillation at moderate-to-high stroke risk. LAAO with the Watchman FLX device was noninferior to DOAC therapy for the composite of stroke, systemic embolism, and cardiovascular death (5.7% vs. 4.8%; posterior probability of noninferiority 97.7%).
For non-procedure-related bleeding, LAAO patients fared significantly better: 10.9% vs. 19.0% (P < 0.001). However, when up-front procedural bleeding was included, overall ISTH major bleeding was comparable (5.9% vs. 6.4%). Importantly, ischemic strokes were numerically more common with LAAO (3.2% vs. 2.2%), a trade-off that warrants careful patient selection.
CHAMPION-AF does not change our approach — it validates it. DOACs remain first-line stroke prevention for atrial fibrillation. They are effective, well-tolerated, and do not require a procedure. That has not changed.
What CHAMPION-AF does establish is that LAAO is a legitimate alternative for the right patient. Who is that? Primarily patients who have experienced significant bleeding on anticoagulation, those with a genuine contraindication to long-term DOAC therapy, and those who — after thorough shared decision-making — prefer a device over a lifetime of daily medication. The reduction in non-procedural bleeding is clinically meaningful for these patients.
The concern is the potential for this trial to be used as justification for LAAO as a first-line replacement for DOACs across the board. That would be a misreading of the data. Noninferiority is not superiority, and a 2.6% procedural complication rate is not zero.
Heart Failure: The Spironolactone Question Persists
Enrolled: 730 of a planned 1,564 patients. The trial was terminated early due to slow enrollment and funding limitations related to the COVID-19 pandemic. The primary endpoint of cardiovascular death or total heart failure hospitalizations was 10.9 per 100 patient-years with spironolactone versus 8.2 with placebo (rate ratio 1.32, 95% CI 0.79–2.21) — numerically favoring placebo, but not statistically significant.
With only 47% of the target enrollment achieved, the trial carried an estimated 65% probability of Type II error — meaning definitive conclusions about efficacy in either direction are impossible from this data.
To be direct: SPIRIT-HF does not answer the question. This was not a true TOPCAT-like trial. TOPCAT enrolled 3,445 patients. SPIRIT-HF managed 730 — under half its own target. Yes, the point estimate numerically favored placebo, but with a 65% probability of Type II error and wide confidence intervals crossing 1.0 in both directions, this trial simply cannot tell us whether spironolactone works or doesn't in HFpEF.
The TOPCAT Americas subgroup remains the best evidence we have, and it showed a 35% reduction in heart failure hospitalization. Until a properly powered trial says otherwise — and SPIRRIT-HFpEF with 6,000+ patients may be the one to watch — spironolactone remains a reasonable option in selected HFpEF patients.
Hypertension: Rethinking the Defaults
In 2,540 stable patients without heart failure or LV dysfunction who had been on beta-blockers for at least 1 year post-MI (median 4.7 years from index MI), discontinuing beta-blockers was noninferior to continuation for the composite of death, recurrent MI, or hospitalization for heart failure: 7.2% vs. 9.0% (HR 0.80, 95% CI 0.57–1.13).
This joins REDUCE-AMI (which found no benefit of starting beta-blockers in preserved EF) in questioning reflexive, indefinite use post-MI. Note that ABYSS failed to meet noninferiority for stopping — so the evidence is evolving, not unanimous. The picture is increasingly clear that beta-blockers deserve individualized scrutiny rather than automatic continuation.
A randomized trial of 176 Black adults with treated hypertension living in Boston-area food deserts. Participants received 3 months of home-delivered DASH-patterned groceries plus dietitian counseling, compared with a grocery stipend plus standard dietary guidance. At 3 months, systolic BP fell 5.0 mmHg more in the DASH delivery group (−7.0 vs. −2.0 mmHg; 95% CI −8.0 to −1.9; P = 0.002), with additional reductions in LDL-C (−7.0 mg/dL). Benefits persisted 3 months after the intervention ended.
This trial demonstrates that making the right dietary choice the easy choice produces measurable results — structural food interventions add real BP benefit on top of medications, and cost less than adding another antihypertensive.
KARDINAL tested tonlamarsen, a novel antisense therapy that directly silences angiotensinogen (AGT) production, in patients with uncontrolled hypertension on two or more medications. Monthly dosing effectively lowered plasma AGT levels, but did not translate into greater blood pressure reductions over 20 weeks compared with a single dose. Strong target engagement, but the BP effect was not yet clinically meaningful. (See ACC.org summary)
Beta-blockers deserve individualized scrutiny, not reflexive prescribing. SMART-DECISION joins REDUCE-AMI in telling us that beta-blockers are not mandatory forever after MI if ejection fraction is preserved. (Note: ABYSS failed noninferiority for stopping — the evidence is evolving but the direction is clear.) This does not mean we stop them in everyone — patients with persistent angina, arrhythmias, or reduced EF still benefit. But the days of automatic lifetime beta-blocker therapy for every post-MI patient should be behind us.
GoFreshRx is a reminder that the fundamentals matter. Before adding pill number four or five for hypertension, are we making it possible for patients to eat well? The DASH diet works — the barrier has always been access and convenience, not evidence.
Other Notable Trials
Pulmonary Embolism
HI-PEITHO enrolled 544 patients with intermediate–high-risk PE across 59 centers and randomized them to ultrasound-assisted catheter-directed thrombolysis (EKOS) plus anticoagulation versus anticoagulation alone. The primary composite of PE-related death, cardiorespiratory decompensation, or symptomatic recurrence was 61% lower in the catheter-directed group at 7 days (P = 0.005; NNT = 16), driven by reduced decompensation — with no excess major bleeding. Published simultaneously in the New England Journal of Medicine.
Hypertrophic Cardiomyopathy
SCOUT-HCM demonstrated that the cardiac myosin inhibitor mavacamten (Camzyos) reduced LVOT gradients in 44 adolescents (ages 12–17) with obstructive HCM over 28 weeks, with improved diastolic function and reduced wall thickness. While small, this is the first Phase 3 trial of this drug class in a pediatric population — published simultaneously in the New England Journal of Medicine.
Putting It All Together
| Trial | Question | Key Result | Practice Impact |
|---|---|---|---|
| Ez-PAVE | LDL-C <55 vs <70 in ASCVD | 33% MACE reduction (HR 0.67, 95% CI 0.56–0.82, P < 0.001) | Practice-confirming |
| CHAMPION-AF | LAAO vs. DOACs | Noninferior; less non-procedural bleeding (10.9% vs 19.0%) | Role for select patients |
| SPIRIT-HF | Spironolactone in HFpEF | Underpowered (47% enrolled); numerically favored placebo, nonsignificant | Question unanswered |
| SMART-DECISION | Beta-blocker discontinuation post-MI | Noninferior (HR 0.80, 95% CI 0.57–1.13) | Individualize therapy |
| VESALIUS-CV | PCSK9i in primary prevention (12,257 pts) | 25% MACE reduction (HR 0.75, P < 0.001); diabetes subgroup 31% (HR 0.69) | First primary prevention PCSK9i trial positive |
| ESSENCE-TIMI 73b | Olezarsen CTA substudy | TG −58–64%; no plaque regression (P = 0.36) | Lipids improved; plaque question open |
| CORALreef AddOn | Oral PCSK9 inhibitor (enlicitide) add-on to statin | 64.6% LDL-C reduction at 8 weeks; 78.2% reached goal | Game-changer for access; outcomes data needed |
| GoFreshRx | DASH grocery delivery in food deserts | −5.0 mmHg SBP (P = 0.002) | Food-as-medicine works |
| HI-PEITHO | Catheter therapy for PE | 61% lower composite endpoint (P = 0.005) | Practice-changing for high-risk PE |
| KARDINAL | Tonlamarsen (antisense AGT) in uncontrolled HTN | AGT lowered; no added BP benefit with repeat dosing | Target engagement, but BP effect unproven |
Final Thoughts
ACC 2026 was a good meeting — not because it overturned our approach, but because it validated it with rigorous evidence. The trials that mattered most were the ones that confirmed what thoughtful clinicians have been doing: pushing LDL-C lower, using LAAO selectively, questioning beta-blocker inertia, and demanding properly powered trials before changing practice. And CORALreef gave us a glimpse of a future where injectable-level LDL-C lowering comes in a pill.
The one disappointment is SPIRIT-HF — not because of its result, but because of its inability to provide one. The question of spironolactone in HFpEF deserves a definitive answer, and 730 patients cannot provide it. We await SPIRRIT-HFpEF.
In the meantime, the CardioAdvocate position remains clear:
- LDL-C: Lower is better. Start earlier. Target <55 mg/dL in ASCVD. Ez-PAVE proved it.
- LAAO: A legitimate option for selected patients — primarily those with bleeding risk or who prefer a device after shared decision-making. DOACs remain first-line.
- Beta-blockers: Individualize. Do not prescribe indefinitely by reflex. Preserved EF post-MI patients can safely discontinue.
- Spironolactone in HFpEF: Still reasonable based on TOPCAT Americas. SPIRIT-HF was underpowered and does not change this.
- Oral PCSK9 inhibitors: CORALreef showed enlicitide achieves injectable-level LDL-C reductions in a pill. Not yet approved, and outcomes data still needed — but the access barrier is falling.
- Finerenone: FDA-approved mineralocorticoid receptor antagonist option with strong evidence in diabetic kidney disease. Consider it — but it's pricey.
CardioAdvocate Rounds
Pull up a chair. We saved you a seat.
Real cases. Real evidence. What we're seeing, what we're missing, and why it matters — delivered to your inbox by a cardiologist who believes everyone deserves a seat at rounds.
Join Rounds →No spam. Unsubscribe anytime. We respect your inbox.
CardioAdvocate helps people understand what matters — and how to speak up about it.
Disclaimer: This Insight Paper reflects the clinical positions of CardioAdvocate based on available evidence as of March 2026 and is intended for educational purposes. It does not constitute individualized medical advice. Treatment decisions should always be made in consultation with your healthcare provider based on individual risk factors, current medications, and personal values. CardioAdvocate does not endorse any specific medication or treatment protocol without consideration of individual patient circumstances. Always evolving. This website is a living document.
CardioAdvocate.com — Founded by Ian Riddock, MD, FACC